A critical and comprehensive review:

In May 2004, a new classification, the RIFLE (Risk, Injury, Failure, Loss of kidney function, and Endstage kidney disease) classification, was proposed in order to define and stratify the severity of
acute kidney injury (AKI). This system relies on changes in the serum creatinine (SCr) or glomerular filtration rates and/or urine output, and it has been largely demonstrated that the RIFLE criteria allows the identification of a significant proportion of AKI patients hospitalized in numerous settings,enables monitoring of AKI severity, and is a good predictor of patient outcome. Three years later (March 2007), the Acute Kidney Injury Network (AKIN) classification, a modified version of the RIFLE, was released in order to increase the sensitivity and specificity of AKI diagnosis. Until now, the benefit of these modifications for clinical practice has not been clearly demonstrated.Here we provide a critical and comprehensive discussion of the two classifications for AKI,focusing on the main differences, advantages and limitations.
Keywords: acute kidney injury; AKIN; RIFLE
Introduction
Over the last few decades, more than 35 different definitions have been used to define acute kidney injury (AKI) [1]. Many of those definitions were complex; however, the more commonly used were based on urine output (UO) and/or serum creatinine (SCr) criteria. An increase in basal SCr of at least 44.2 μmol/L (0.5 mg/dL), a decrease in Cr clearance of at least 50% or the need for renal replacement therapy (RRT) were the most frequent definitions used for AKI in clinical practice [2]. Where UO has been used to define AKI, it is generally considered that a value less than 400–500 mL/day could be an indicator. Multiple definitions for AKI have obviously led to a great disparity in the reported incidence of AKI making it difficult or even impossible to compare the various published studies focusing on AKI [3–7]. Therefore, it became crucial to establish a consensual and accurate definition of AKI that could ideally be used worldwide.The RIFLE classification
In May 2002, the Acute Dialysis Quality Initiative (ADQI) group for the study of AKI, composed of nephrologists and intensivists, came together over 2 days in a conference in Vicenza (Italy), with the purpose of defining AKI.From this conference, the consensual RIFLE (Risk, Injury,Failure, Loss of kidney function, and End-stage kidneydisease) classification for AKI definition emerged, whichwas published in May 2004 in Critical Care [8].
The ADQI group considered that the ideal AKI definition
would have to accomplish the following criteria: easy clinical applicability, sensitivity and specificity, consider baseline SCr variations and also consider the ‘acute-on-chronic’phenomenon (which means the occurrence of an acute insult over a chronically injured renal function causing its
deterioration). This definition should classify AKI according to its severity (mild versus severe) and its timing of occurrence (precocious versus late AKI). By fulfilling these criteria, this classification should allow the detection of patients whose kidney function was slightly affected (high
sensitivity but low specificity) as well as patients with severe kidney function deterioration (high specificity with diminishing sensitivity).
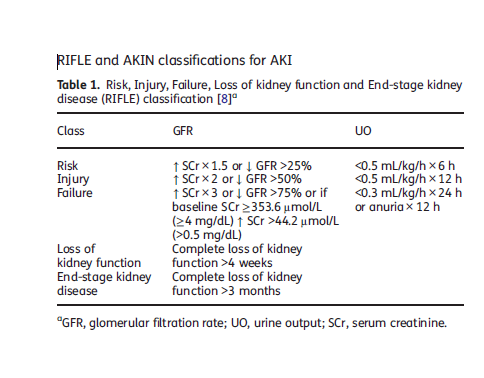
The RIFLE classification (Table 1) is based on SCr and UO determinants, and considers three severity classes of AKI (Risk, Injury and Failure), according to the variations in SCr and/or UO, and two outcome classes (loss of kidney function and end-stage kidney disease). The patient should be classified using the criteria (SCr and/or UO) which leads to the worst classification (maximum
RIFLE), for instance, if a patient was in the Risk class according to the UO but in the Injury class according to SCr variation, then the worst criteria (SCr) should be used for classifying the severity of AKI in this patient.
The temporal pattern of the SCr and/or UO variation is also relevant for defining AKI: the deterioration of renal function must be sudden (1–7 days) and sustained (persisting >24 h).
This definition can easily be applied when the baseline SCr is known; however, in a significant number of patients baseline SCr is unknown; in these cases, if there is no history of chronic kidney disease (CKD), baseline SCr should be calculated using the Modification of Diet in Renal Disease (MDRD) [9] equation, assuming a baseline glomerular filtration rate (GFR) of 75 mL/min/1.73m2.
Strengths and limitations of the RIFLE classification Strengths of the RIFLE classification. RIFLE has been largely validated in terms of determining the incidence of AKI and its prognostic stratification in several settings of hospitalized patients [10–26].
In these studies, RIFLE facilitated the identification of a large proportion of AKI patients and there was an independent and stepwise increase in mortality as AKI severity increased; RIFLE also exhibited a good prognostic accuracy in terms of mortality (Table 2). Furthermore, it has been shown that the RIFLE enables monitoring of the progression of AKI severity during hospitalization and
RIFLE classes are strongly associated with increased lengths of stay, RRT requirement, renal function recovery and discharge from hospital to a care facility [11–14, 26].
Originally, the RIFLE criteria was established to standardize the definition and stratification of AKI severity. Several studies, however, have determined the ability of the RIFLE in predicting mortality using the area under the receiver operating characteristic (AUROC) curve, and some of them have inclusively compared it with other general or specific scoring systems [16, 17, 21, 23, 24, 27, 28]. Taking into account that the RIFLE relies only on renal function it would be conceivable that the RIFLE prognostic capacity was inferior to that of other general scores (i.e. Acute Physiology and Chronic Health Evaluation,Simplified Acute Pathophysiology Score). However, RIFLE has proven to be an important tool in predicting patient outcome and, furthermore, seems to have increased the prognostic ability of those general scores usually employed in the intensive care unit (ICU).
Limitations of the RIFLE classification. Despite its clinical use, the RIFLE classification has a number of important limitations. First, baseline SCr is necessary to define and classify AKI; this baseline value is frequently unknown in clinical practice. In this situation, the ADQI work group [8]
propose estimating the baseline SCr using the MDRD equation [9], assuming a baseline GFR of 75 mL/min/1.73m2. In CKD patients, baseline SCr determined assuming a GFR of 75 mL/min/1.73m2 has a low correlation with the real value of SCr and results in an overestimation of AKI incidence [29]. Second, the MDRD formula has been validated in CKD patients with stable renal function,
not in AKI patients.
Third, in several of the studies previously mentioned, only SCr was used to define and stage AKI [12, 15, 20]. In CKD patients, compared with patients with previously normal renal function, the percentage increase in SCr used to define AKI generally occurs later and, thus, defining AKI using only the SCr criteria could diminish the sensitivity of AKI diagnosis in CKD
patients [30].
Moreover, determination of renal function using SCr has several other limitations as listed below:
- The endogenous production and serum release of Cr are variable, and it is influenced by multiple factors, namely age, gender, diet, and muscle mass;
- 10 to 40% of Cr elimination is performed by tubular secretion [31] and this mechanism is amplified as the GFR diminishes, thus, overestimating renal function in AKI patients;
- many medications inhibit tubular secretion of Cr (i.e. trimethoprim, cimetidine), causing a temporary increase in SCr;
- various factors can interfere with SCr determination (i.e. acetoacetate accumulated in diabetic ketoacidosis can interfere with the alkaline picrate method), causing a false elevation in SCr [32];
- Cr is a marker of renal function, and not of renal lesion.
(i) Sensitivity and specificity of UO can be significantly changed by the use of diuretics, and this issue is not specifically considered in the RIFLE classification;
(ii) the UO can only be determined in patients with a bladder catheter in place, which, despite being
common in ICU patients, is not frequent in other hospitalized patients;
(iii) It is possible that the predictive ability of UO could be inferior to that of SCr, which can explain the difference in terms of mortality between the same classes defined by each one of those criteria, observed in studies that utilized both criteria to define and classify AKI [11, 13, 34]. The capacity of the RIFLE (using both criteria) to predict mortality can be more stable than the ability of this classification employing only SCr [13, which corroborates the clinical utility of using simultaneously both criteria as proposed by the ADQI work group [8].
Fifth, the aetiology of AKI and the requirement for RRT are not considered in the RIFLE classification. In two studies that evaluated ICU patients with AKI requiring continuous RRT, the RIFLE classification showed less acuity in predicting mortality [35, 36]. One possible explanation
 for this phenomenon is that in both the studies, the clinical severity of patients was so high that it could not allow RIFLE to discriminate mortality according to AKI severity (i.e. between the three classes).
for this phenomenon is that in both the studies, the clinical severity of patients was so high that it could not allow RIFLE to discriminate mortality according to AKI severity (i.e. between the three classes).Finally, the RIFLE classification does not provide any information regarding the origin of the renal lesion (i.e. cellular or subcellular levels), as opposed to several biomarkers of AKI recently identified and studied. Furthermore,the limitations of the conventional renal function markers (Cr and UO) can be overwhelmed with the utilization of those new biomarkers. In fact, various urinary and serum markers of AKI have been identified and described [37], such as neutrophil gelatinase-associated
lipocalin, interleukin-18 and the kidney injury molecule-1. These biomarkers start to elevate soon in AKI (1–3 days before the increase in SCr), and do exhibit a great sensitivity and specificity in AKI diagnosis, a good correlation with RRT requirement, as well as with mortality, in several settings, namely in the post-operative period of cardiac surgery [38, 39], in ICU patients [40] and in the contrastinduced nephropathy in children undergoing coronary angiography [41]. In renal transplantation, it has been shown that these biomarkers also have a good correlation with the cold ischaemic time, the maximum value of SCr in the post-transplantation period and the requirement
for RRT, and are good predictors of acute tubular necrosis and long-term renal graft function [42, 43, 44].
It must also be emphasized that the RIFLE criteria has only has only evaluated in a minority (<2%) of patients included in prospective studies. This major concern certainly did limit the analysis of other clinical or laboratory variables with prognostic impact on the epidemiology of AKI.
The Acute Kidney Injury Network (AKIN) classification
In September 2005, in a meeting in Amsterdam a new classification of AKI was proposed by the Acute Kidney Injury Network (AKIN) working group composed of nephrologists, critical care physicians and other physicians specialized in AKI.
The AKIN classification (Table 3) was published in March 2007 in Critical Care [45], and it is a
later version of the RIFLE classification with some modifications:
the diagnosis of AKI is only considered after achieving an adequate status of hydration and after
excluding urinary obstruction; the AKIN classification only relies on SCr and not on GFR changes; baseline SCr is not necessary in the AKIN classification, and it requires at least two values of SCr obtained within a period of 48 h;
AKI is defined by the sudden decrease (in 48 h) of renal function, defined by an increase in absolute SCr of at least 26.5 μmol/L (0.3 mg/dL) or by a percentage increase in SCr ≥50% (1.5× baseline value), or by a decrease in the UO (documented oliguria <0.5 mL/kg/h for more than 6 h);
Stage 1 corresponds to the risk class, but it also considers an absolute increase in SCr ≥26.5 μmol/L (0.3 mg/dL);
Stages 2 and 3 correspond to injury and failure classes, respectively;
Stage 3 also considers patients requiring RRT independently of the stage (defined by SCr and/or UO) they are in at the point of RRT
initiation; the two outcome classes (loss of kidney function and end-stage kidney disease) were removed from the classification.

It has been shown that the AKIN classification, like the RIFLE classification, allowed the identification and stratification of AKI in a large proportion of hospitalized patients and was independently associated with the outcome [34, 48–56]. In fact, patients with AKI had higher in-hospital mortality and longer lengths of stay, and AKI survivors were more likely to be discharged to an extended care facility.
The AKIN classification could theoretically improve the RIFLE criteria sensitivity and specificity, although the advantages of the RIFLE modifications have not been proven. In fact, the AKIN classification compared with the RIFLE classification did not exhibit a better prognostic acuity in terms of in-hospital mortality, although it enabled the identification of more AKI patients.
Strengths and limitations of the AKIN classification
The AKIN classification is a modified version of the RIFLE classification; therefore, their strengths and limitations are very similar to those aforementioned for the RIFLE.
The AKIN classification has, however, some additional benefits and limitations related to the modifications introduced to the RIFLE classification.
Strengths of the AKIN classification.
First, the AKI definition is only considered after an adequate status of hydration is achieved. Therefore, the AKIN classification,unlike RIFLE, adds important aetiological information.
Second, the AKIN classification is based on SCr and not on GFR changes.
Third, the AKIN classification does not need baseline SCr to define AKI, although it requires at
least two SCr determinations within 48 h.
Limitations of the AKIN classification.
First, the AKIN classification does not allow the identification of AKI when SCr elevation occurs in a time frame higher than 48 h.
Second, Stage 3 of the AKIN classification includes three diagnostic criteria (Cr, UO and RRT requirement),and the extreme variability in the beginning and cessation of RRT as well as in RRT modality used and in the dose of dialysis among different physicians, hospitals and countries could significantly limit the prognostic acuity of this classification, particularly of Stage 3.

Which classification should we use in clinical practice?
The extensive number of publications focusing on the RIFLE and AKIN classifications are demonstrative and they are widely accepted by the medical community. There remains, however, some heterogeneity in the utilization of the criteria defining and classifying AKI, such s the use (or non-use) of UO and baseline SCr, and of the estimated GFR instead of the variation in SCr.The Kidney Disease Improving Global Outcomes work group recently combined the RIFLE and AKIN classifications in order to establish one classification of AKI for practice, research and public health.
Therefore, AKI has been defined as an increase in SCr ≥0.3 mg/dL (≥26.5 μmol/L) within 48 h; or an increase in SCr to ≥1.5 times baseline, which is known or presumed to have occurred within the prior 7 days or a urine volume of <0.5 mL/kg/h for 6 h.
Furthermore, AKI has been staged in severity according to the AKIN criteria (Table 3).
One additional change in the criteria was made for the sake of clarity and simplicity.
For patients reaching Stage 3 by SCr >4.0 mg/dL (>354 μmol/L), rather than requiring an
acute increase of ≥0.5 mg/dL (≥44 μmol/L) over an unspecified time period, it instead require that the patient first achieve the creatinine-based change specified in the definition [either ≥0.3 mg/dL (≥26.5 μmol/L) within a 48-h time window or an increase of ≥1.5 times baseline]. This change brings the definition and staging criteria to greater parity and simplifies the criteria [57].
The integration of the new biomarkers of AKI into the clinical classification could increase the sensitivity and specificity of AKI diagnosis, overwhelming some of the limitations of the traditional
markers of kidney function, such as Cr and UO [58].
Downloaded from http://ckj.oxfordjournals.org/ by guest on May 28, 2015







{kind=link}